
Scientific journal
European Journal of Natural History
ISSN 2073-4972
ИФ РИНЦ = 0.204
FEATURES OF CLINICAL COURSE AND EFFICACY OF TREATMENT FOR HYPOTHYROID GOITER DEPENDING ON STRENGTH OF EXCITATION IN THE CENTRAL NERVOUS SYSTEM

Based on the guideline of Russian pathophysiologists Gorizontov et al., published in 1966, we know that the clinical course of many diseases, as well as the effectiveness of their therapy, ultimately depends on character of individual reactivity and nonspecific resistance, which are conditioned by constitutional features of an organism and, foremost, the nervous system [5].
Several studies, conducted by Yepisheva (1992), Artyomov (1993), and Khodjaeva (1999), have found that individuals with strong manifestation of excitation process of the nervous system (strong, balanced and mobile processes in the central nervous system (CNS)) have much easier and faster course of disease and high efficiency of therapy due to higher stress tolerance and productivity of immune response, compared with representatives with less significant excitation processes in the CNS (weak and unbalanced neurological processes) [2, 7, 11].
According to Little (2006), the thyroid disorders affect many body systems, which lead to a serious disturbance of the majority of homeostatic parameters [8]. Subsequently, both in terms of prognostication of hypothyroid goiter and improve the effectiveness of treatment, it would gain the undoubted importance the study of dependence of clinical course of hypothyroid goiter on the basic properties of the CNS as power of excitation, on which individual reactivity depends.
Recently published evidence-based studies by Kaplan et al. (2003), Escobar-Morreale et al. (2005), and Santini et al. (2005) reported efficacy of long-term administration of thyroxine in the treatment of hypothyroid states. As a rule, the success of therapy is based on the correct selection of doses, and depends on many factors such as age, pregnancy, nutritional factors, comorbidity et al. [3, 6, 10]. Meier et al (1993) noted that the most important of them is individual sensitivity of organism [9], which is still not well studied.
In this occasion, the aim of our research was to study features of clinical course and efficacy of treatment for hypothyroidism, depending on the strength degree of excitation in the CNS.
Materials and methods of research
Our study is based on results of dynamic management and treatment of 86 patients with manifesting (symptomatic) form of hypothyroidism aged from 17 to 60 years old. Duration of the disease varied between 1-7 years.
Using the «Temping test» by Ilyin E.P. (2004), we determined the strength degree of excitation in the CNS. This test consists in counting the number of pushes on the button for several 5-second intervals, followed by forming graphics, where on the horizontal axis marked time intervals, and on the vertical one - the number of pushes in each interval. The test was carried out multiple times as on the primary admission of patients to the hospital, and after they achieve euthyroid state. The test results were taken into account, when they coincided in no less than 75 %. For further research, we selected two marginal variants of expression of excitation processes (EEP) in the CNS: «strong», which is characterized by a convex or rising type of curve, and «weak» with a descending type of graphics.
The study of hormonal background (thyrotropin, total triiodothyronine (T3) and total thyroxine (T4)) was performed by immunoenzimatic method using sets of firm «Human». Achilles reflex time was expanded by reflexometer «Achill-01».
To determine the functional state of the thyroid gland, we have proposed a table consisting of 5 groups of symptoms related to specific body systems. The appropriate number of points assesses the presence or absence and severity of each symptom. In this case, similarly are estimated the quantitative measures of pulse and blood pressure. In general, the value of total score can range from 0 to 105 points and indicates to hyperthyroid state at values above 65 points, euthyroid status - in the range 35-65 points, and hypothyroid - when values are less than 35 points (table).
Severity of thyroid symptoms, in points (scores)
|
№ |
Symptoms |
Absence (score) |
Availability (score) |
||||
|
Reduced |
Average |
Strengthened |
Extremely strengthened |
||||
|
CNS |
1 |
Personality (reaction to environment) |
Apathy (0) |
Inhibited consciousness (1) |
Norm (2) |
Irritation (4) |
Nervousness (6) |
|
2 |
Sleep |
Drowsiness (0) |
Daytime sleepiness (2) |
Norm (4) |
Restless (5) |
Insomnia (6) |
|
|
3 |
Motor reactions (action) |
Very slowly (0) |
Slow (1) |
Norm (2) |
Fussiness (3) |
Excessive fussiness (4) |
|
|
4 |
Speech |
- |
Slow (0) |
Norm (1) |
Fast (2) |
- |
|
|
5 |
Tremor |
No (0) |
- |
- |
In the hands (3) |
In whole body (6) |
|
|
6 |
Sweating |
- |
Not marked (0) |
Norm (3) |
Excessive (6) |
- |
|
|
7 |
Feeling the heat |
- |
Feeling cold (0) |
Norm (2) |
Feeling hot (3) |
- |
|
|
SKIN |
8 |
Skin color |
Icteric (0) |
Pale (2) |
Norm (4) |
Hyperemia (6) |
- |
|
9 |
Skin moisture |
Flaked off (0) |
Dry (2) |
Norm (4) |
Moist (6) |
- |
|
|
10 |
Skin thickness |
- |
Thick (0) |
Norm (3) |
Thin (6) |
- |
|
|
CVS |
11 |
Pulse (times per min |
< 50 (0) |
50-69 (3) |
70-80 (6) |
81-100 (9) |
> 101 (14) |
|
12 |
Systolic blood pressure (mm Hg) |
<89 (0) |
90-109 (1) |
110-120 (2) |
121-140 (4) |
> 141 (6) |
|
|
13 |
Diastolic blood pressure (mm Hg) |
- |
< 70 (0) |
70-80 (1) |
81-100 (2) |
>101 (3) |
|
|
14 |
Heart sounds |
- |
Muffled (0) |
Clear (2) |
Sonorous (4) |
- |
|
|
Gastrointestinal tract |
15 |
Appetite |
- |
Decreased (0) |
Norm (1) |
Increased (3) |
- |
|
16 |
Stool disorders |
Constipation (0) |
Tendency to constipation (2) |
Norm (4) |
Unstable, < 3 per day (6) |
Unstable, > 3 per day (8) |
|
|
17 |
Body weight |
Increased by obesity and edema (0) |
Increased due to obesity (2) |
Norm (4) |
Decreased <20% of initial for 3 months (6) |
Decreased >20% for 3 months (8) |
|
|
Eyes |
18 |
Glance |
- |
Dim (0) |
Norm (2) |
Eye-shine (5) |
- |
|
19 |
Exophthalmus |
- |
- |
No (0) |
- |
Exists (2) |
|
For the treatment of manifesting hypothyroidism, we used thyroid preparations (L-thyroxine, euthyrox) from initial dosage of 1,6 mg/kg body weight to normalize thyrotropin levels with a further selection of individual maintenance dose.
Results of research and their discussion
Figure shows that pattern of clinical symptoms in patients varied depending on the strength degree of excitation in initial condition.
Examination of patients before treatment showed that the hypothyroid state is accompanied by a significant decrease in total score of clinical symptoms. It was found that if patients with strong EEP had total score reached up to 21,3 units, then in those with weak EEP it was up to 15,3 units.
During the first 2 months of treatment with thyroxine, significant positive dynamics of clinical symptoms (total increase of more than 12 points) was observed in patients with strong excitation processes in the CNS, whereas in the other group this index was 2 times less. However, over the next 2-month course of hormonal therapy, dynamics of clinical symptoms become manifest in both groups to the same extent (increase by 8-9 points). Moreover, if patients with expressed manifestation of excitation process in the CNS reached the lower limit of euthyroid state (35 points) after 2 months of therapy, then patients with weak EEP obtained this result only after 6 months. Later, after 4 months for patients with strong EEP and 8 months for those with weak EEP, the values of total score of clinical symptoms start to stabilize. However, even while the groups achieved their respective maximum values, the differences between them on this index was at least 4 points.
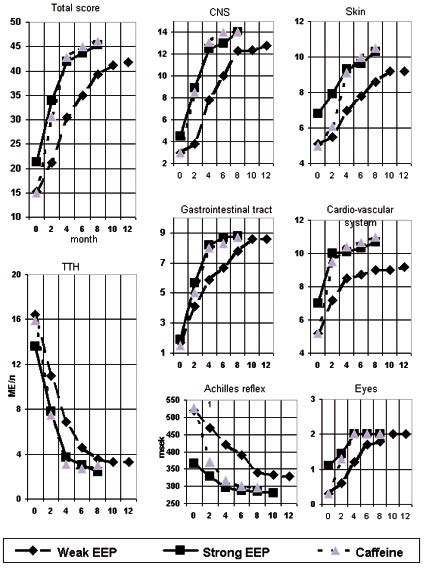
Changes in clinicalsigns during the treatment of patients with hypothyroidism with different expression
of excitation processes (EEP)
Initial differences in the total score in accordance with EEP in the CNS caused by the manifestation of clinical signs mainly of the cardiovascular system (CVS), CNS and skin (2 points), as well ocular symptoms, but to a lesser extent. Treatment of patients with strong EEP resulted in sharp increase in the number of points with achievement of euthyroid state limits in 2 months for the CVS and 4 months for other symptoms. Patients with weak EEP were characterized by some delay during the first 2 months followed by further intensive increase in the number of points of clinical signs of the CNS and skin symptoms, which similar to above group. Furthermore, when patients with strong EEP achieved the euthyroid state, it was observed some predominance of the number of points in all clinical signs, save for ocular.
Thus, symptoms of the CNS are observed to change most significantly, depending on the strength of excitatory processes in the CNS. To determine possible links between them, we also studied indicators of Achilles reflex duration, which reflects manifestation of excitation processes in somatic nerves.
Figure 1 demonstrates that clear difference in reflex duration between the groups of patients with different EEP was identified already in initial state. In representatives with weak EEP, its average value exceeds 500 milliseconds, whereas in those with strong EEP it was almost a third less (P < 0,001). Up to 4-month period of treatment reduction rate in reflex duration was the similar in both groups, but by that time, in those with strong EEP, this parameter reached the normal parameters (below 300 milliseconds) and further were observed no significant changes. Minimum values in this index in patients with weak EEP were gained only after 8 months of treatment, and subsequently did not decrease below 325 milliseconds (on average by 50 milliseconds greater than for the persons with strong EEP).
In hypothyroid states, change in the level of thyrotropin is known to have the important diagnostic value. In general, before treatment in patients with weak excitation processes this parameter was an average of 3 nmol/L higher than in compared group (P < 0,05), and amounted 16,5 ± 1,4 nmol/L (Figure). During the 4-month treatment, thyrotropin levels in all patients decreased to the same extent, and initial differences between the groups remained. However, this parameter in patients with strong EEP by this time settled in the normal range, and achieved normal levels only after 8 months of hormonal therapy. Although, further levels of thyrotropin in both groups were no significantly changed, however the differences between them remained within a mean of 1,2 nmol/L.
Along with this, changes in levels of T3 and T4 did not depend on the degree of excitation processes in the CNS, both before and during the treatment of patients.
In general, more severe clinical symptoms of hypothyroidism ab initio and less effective treatment are observed in patients with weak EEP. If it is indeed associated with the peculiarity of the CNS functioning, so the strengthening of excitation by any medications should have a significant effect on the disease course. We suppose that for this purpose the most suitable may be caffeine, which has the ability to increase the excitation processes in the CNS and is widely consumed in the tea and coffee. Assuming that the consumption of caffeine in the drinks will not be enough to achieve the approximate indicators of nervous system functioning in individuals with weak EEP to that in those with strong EEP, we introduced into complex treatment of patients with hypothyroidism caffeine in a daily dose of 1,5 grams.
According to change in total score of clinical symptoms, this drug significantly reduced the time required to achieve the euthyroid state (from 8 to 4 months) (Figure). This was due to the rapid and complete disappearance of clinical neurological symptoms, when after 2 months of treatment with caffeine the parameters in patients with weak EEP almost did not differ from patients with strong EEP. The similar tendencies were observed in CVS, gastrointestinal and eye symptoms. Only on the dynamics of cutaneous symptoms such pattern was somewhat later - after 4 month. Such changes were observed for indicators of the Achilles reflex, but after a two-month period, the differences between patients with strong and weak EEP under the influence of the drug lost statistical significance.
For the full evaluation of results it should be clarified whether identifying clinical changes caused by increased levels of thyroid hormones or by tissues sensitivity to them. Studies showed that the administration of caffeine to thyroxine replacement therapy had no significant effect on T3 and T4 levels. At same time, the drug reduced the timeframe for achieving euthyroid state in thyrotropin level almost in 2 times, and its dynamics from the second month did not differ from the indexes of patients with strong EEP (Figure).
Summary
According to results obtained, clinical manifestations of hypothyroidism depend on the EEP strength: CNS, CVS, skin and eye clinical symptoms were more expressed at weak excitation processes in the CNS. At same time, the absence of differences in reduction of thyroid hormones levels indicates a lower sensitivity of tissues and organs to hormonal deficiency in patients with strong EEP. We think that this is confirmed to some extent by the lower values in thyrotropin level and duration of Achilles reflex in these patients. Correction the deficit of thyroid hormones through hormone replacement therapy resulted in reduction of clinical symptoms and achievement of euthyroid state, which was almost 2 times slower and somewhat less expressed in weak EEP, despite similar changes in the levels of thyroid hormones (T3 and T4) in blood of all patients. We consider that the data obtained, probably, can be explained by the lower need of organism with strong EEP in thyroid hormones for the maintenance its stable euthyroid state, as well as by less sensitivity to their deficit, accordingly.
Thus, to answer the question «is it has a direct relation to intensity of excitation processes in the CNS or is it only connected with any other factors», we additionally stimulated the CNS of patients with weak EEP by caffeine. In this case, strengthening of excitation processes contributed to manifestation of changes in studied parameters similarly to patients with strong EEP. According to the literature1 and our own study, this testifies to an inverse relationship of excitation intensity in the CNS, and tissue need for thyroid hormones.
References
- Akmaev I.G. Interaction between nervous, endocrine and immune mechanisms of brain // Journal of Neurology and Psychiatry. - 1998. - №3. - Р. 54-56.
- Artyomov A.P. The value of typological and biochemical characteristics of an organism of the patients with drug and toxin abuse for the determination of risk factors and clinical course of the disease, Abstract of the thesis for PhD. - Tashkent (Uzbekistan), 1993. - 18 p.
- Escobar-Morreale H.F., Botella-Carretero J.I., Gomez-Bueno M. et al. Thyroid hormone replacement therapy in primary hypothyroidism: a randomized trial comparing L-thyroxine plus liothyronine with L-thyroxine alone // Journal of Ann. Intern. Med. - 2005. - Vol. 142. - Р. 412-424.
- Gorizontov P.D., Mayzelis M.Y. Importance of constitution for the development of diseases, Multivolume guide on Pathophysiology. - M.: Medicine, 1966. - Р. 286-319.
- Kaplan M.M., Sarne D.H., Schneider A.B. In search of the impossible dream? Thyroid hormone replacement therapy that treats all symptoms in all hypothyroid patients // Journal of Clin. Endocrinol. Metab. - 2003. - Vol. 88. - Р. 4540-4542.
- Khodjaeva R.Sh.. Individualization of treatment of patients with hypertonic disease, depending on the type of nervous system, hemodynamics and pharmacologic metabolizing characteristics of an organism, Abstract of the thesis for PhD. - Tashkent (Uzbekistan), 1999. - 19 p.
- Little J.W. Thyroid disorders. Part II: hypothyroidism and thyroiditis // Journal of Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. - 2006. - Vol. 102. - Р. 148-153.
- Meier C.A., Maisey M.N., Lowry A. et al. Interindividual differences in the pituitary-thyroid axis influence the interpretation of thyroid function tests // Journal of Clin. Endocrinol. Metab. - 1993. - Vol. 39. - Р. 101-107.
- Santini F., Pinchera A., Marsili A., et al. Lean body mass is a major determinant of levothyroxine dosage in the treatment of thyroid diseases, Journal of Clin. Endocrinol. Metab. - 2005. - Vol. 90. - Р. 124-127.
- Yepisheva L.V. Pathogenetic therapy of atopic dermatitis in children: the importance of features of typology of nervous system, autonomic reactivity, phenotype of acetylation and monooxygenases activity, Abstract of the thesis for PhD. - M., 1992. - 17 p.
Библиографическая ссылка
Mukhtarova M.Z, Karimov K.Y, Ashirmetov A.H FEATURES OF CLINICAL COURSE AND EFFICACY OF TREATMENT FOR HYPOTHYROID GOITER DEPENDING ON STRENGTH OF EXCITATION IN THE CENTRAL NERVOUS SYSTEM // European Journal of Natural History. 2011. № 3. ;URL: https://world-science.ru/en/article/view?id=27987 (дата обращения: 27.07.2026).