
Scientific journal
European Journal of Natural History
ISSN 2073-4972
ИФ РИНЦ = 0.204
APPLICATION OF THE MELD SCALE TO ASSESS THE SEVERITY OF LIVER CIRRHOSIS IN THE OUTCOME OF CHRONIC HEPATITIS C IN THE KYRGYZ REPUBLIC

Viral hepatitis is one of the leading causes of death in the world, which until recently was not given sufficient attention as a priority public health problem. It is estimated that in the European region of the World Health Organization (WHO), about 171 000 people die annually from causes related to viral hepatitis (approximately 2% of all deaths), which corresponds to more than 400 deaths per day. Approximately 98% of these deaths are caused by long-term consequences of chronic viral hepatitis B and C, such as liver cirrhosis and hepatocellular carcinoma (HCC).
A high frequency of liver cirrhosis formation was established in the outcome of chronic viral hepatitis C genotype 1b [1-3]. According to observations, the frequency of liver cirrhosis formation in patients with chronic viral hepatitis C (HCV) caused by various HCV genotypes have values close to each other [4, 5]. Conflicting information regarding genotypes HCV, which play a leading role in the development of liver cirrhosis, require further research.
Cirrhosis of the liver of viral origin has a very high rate of progression, which determines a shorter life expectancy, so, 5 years after diagnosis, the mortality rate reaches 70%. In the USA, 4 million people are infected with the chronic HСV, in 80-85% of cases, cirrhosis of the liver may develop in the future, but at the same time, in approximately 10-20% of cases, the cause of cirrhosis of the liver cannot be established.
In economically developed countries, cirrhosis of the liver is among the six most common causes of death in patients aged 35 to 60 years, accounting for 14-30 cases per 100 thousand population [6].
In the Kyrgyz Republic, the prevalence of cirrhosis of the liver over a 10-year period increased from 30,60/0000 (2008) to 37,6 0/0000 (2017) (1,3 times). The largest changes in indicators were observed in the southern region of the republic, so, in the Jalal-Abad region, the values increased by 1,9 times during this period. Of great concern is the high mortality rate among the able-bodied population and the increase in the number of cases of disability, in general, in the republic by 1,2 times and by 1,2-1,4 times in the regions [7, 8, 9].
In this regard, at present, an urgent task in the Kyrgyz Republic is to timely assess the severity of liver cirrhosis, further predict the survival and mortality of patients, as well as to plan the selection of patients for liver transplantation.
The high rates of liver cirrhosis in the republic, the increase in disability and mortality among the able-bodied population served as the basis for this study to develop timely adequate therapeutic and diagnostic measures.
Purpose of the study. Assessment of the severity of the disease and the prognosis of life in patients with cirrhosis of the liver in the outcome of chronic viral hepatitis C on the MELD scale.
Materials and methods of research
To determine the MELD scale, 107 patients with subcompensated cirrhosis of the liver according to the severity of Child-Pugh class B (n=68), decompensated cirrhosis of the liver according to the severity of Child-Pugh class C (n=39) in the outcome of chronic viral hepatitis C aged 25 to 60 years were examined.
To assess the severity of liver cirrhosis and the prognosis of survival in the patients we observed, as well as to determine the priority of candidates for liver transplantation, we used the MELD (Model for End – Stage Liver Disease) calculation scale developed using regression analysis in the USA, in which the degree of renal dysfunction is taken into account during the assessment of portal hypertension parameters [10, 11, 12].
The calculation of this indicator includes the level of bilirubin, serum creatinine, as well as the level of INR (international normalized ratio). Calculated using the following formula:
MELD = 11.2 x ln (INR) + + 9.57 x ln (creatinine, mg/dl) + +3.78 x ln (bilirubin, mg/dl) + 6.43
Statistical processing of the results of the study was carried out using the Microsoft Excel 2016 program. The correlation analysis was carried out with the calculation of the Pearson correlation coefficient. The reliability of the differences was determined by the Student’s t criterion.
Results of the research and discussions
Considering that our patients were at different stages of the disease, we were interested in exploring the possibility of using the MELD scale to assess the severity of liver cirrhosis in the outcome of chronic hepatitis C, predict an unfavorable outcome in patients with end-stage liver cirrhosis, and also use it in patients awaiting liver transplantation.
In the observed patients with decompensated liver cirrhosis, the levels of total bilirubin, creatinine and the International Normalized Ratio index (INR) were significantly higher than in the subcompensated stage of class B liver cirrhosis on the Child-Pugh scale. The average score, according to the MELD scale, in the analyzed patients significantly increased with an increase in the severity of cirrhosis of the liver in the outcome of HCV. In the subcompensated stage of liver cirrhosis, the MELD index was 15±1,66 points, and in the decompensated stage of the disease – 25±0,8 points (p<0.001) (table 1).
In all the observed patients, we calculated the correlation coefficient between the index of the MELD scale and the levels of albumin and globulin.
As can be seen from fig. 1, there is an inverse correlation at the average level between the albumin content in the blood and the MELD scale index (r = – 0,69), so lower albumin level was associated with higher values of the MELD scale.
A statistically significant correlation was also noted between the level of MELD and the level of γ-globulin. As can be seen in fig. 2 there is a positive strong correlation between the level of γ-globulin and the values of the MELD scale (r = 0,73).
In patients with an increased AFP index, the correlation with the MELD index was studied. An average correlation was found between the AFP level and the MELD index (r = 0,59) (Fig. 3). In the observed patients, an increased level of AFP was associated with a higher MELD index. At the same time, a correlation between the MELD index and AFP was observed, but not always.
Table 1
Assessment of the severity of liver cirrhosis in the outcome of chronic viral hepatitis C on the MELD scale (n=107)
|
Indicators |
Subcompensated cirrhosis of the liver Class В (n=68) |
Decompensated cirrhosis of the liver Class С (n=39) |
P |
|
Total bilirubin, mmol/l |
26,7±1,8 |
38,9±1,6 |
p < 0,001 |
|
International normalized attitude, un.(N=0,8-1,2) |
1,7±0,05 |
2,20±0,32 |
p > 0,05 |
|
Creatinine, mmol/l |
95,2±2,5 |
169,0±10,1 |
p < 0,001 |
|
MELD, points |
15±1,66 |
25±0,8 |
p < 0,001 |
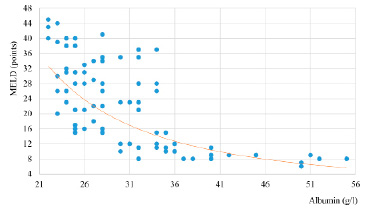
Fig. 1. Correlation between the albumin index and the values of the MELD scale, r = – 0,69 (n=107)
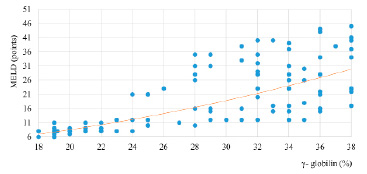
Fig. 2. Correlation of the γ-globulin index and the values of the MELD scale, r = 0,73 (n=107)
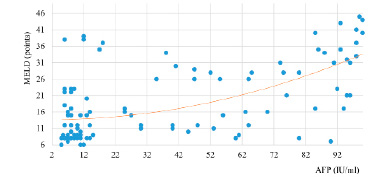
Fig. 3. Correlation of AFP and MELD indicators, r = 0,59 (n=107)
Table 2
Prognostic assessment of 3-month survival of patients with cirrhosis of the liver in the outcome of HCV in the stages of subcompensation and decompensation (class B and C according to Child-Pugh) by MELD scale (n=107)
|
№ |
MELD score |
survival, % |
Subcompensated cirrhosis of the liver Class В (n=68) |
Decompensated cirrhosis of the liver Class С (n=39) |
||||
|
Patients, abs. qty |
Survival, abs. qty |
Lethality, abs. qty |
Patients, abs. qty |
Survival, abs. qty |
Lethality, abs. qty |
|||
|
1 |
<=10 |
98,1% |
35 |
34 |
1 |
- |
- |
- |
|
2 |
11-19 |
94,0% |
16 |
15 |
1 |
13 |
12 |
1 |
|
3 |
20-29 |
80,4% |
8 |
6 |
2 |
12 |
10 |
2 |
|
4 |
30-39 |
47,4% |
6 |
3 |
3 |
10 |
5 |
5 |
|
5 |
>=40 |
28,7% |
3 |
1 |
2 |
4 |
1 |
3 |
|
TOTAL |
68 |
60 |
8 |
39 |
28 |
11 |
||
The data obtained make it possible to predict the severity of the content of these components in the blood, identify possible candidates for liver transplantation, or outline treatment tactics and necessary medications.
Thus, a higher MELD index in the subcompensated stage of liver cirrhosis of class B, determined by the Child-Pugh scale, and the decompensated stage of liver cirrhosis of class C on the Child-Pugh scale is observed in patients with low albumin levels and high levels of γ-globulin and AFP.
The value of the MELD index in our study ranged from 1 to 44 points. To interpret the data obtained, the MELD index uses the prognosis of survival depending on the follow-up period and complications in patients. To predict the survival of patients with cirrhosis of the liver in the outcome of HCV, we used the recommended survival values for a 3-month period (Table. 2), since, when using 6 and 12 month survival rates, a large percentage of mortality is obtained for classes B and C on the Child Pugh scale. Therefore, for patients in the stages of subcompensation and decompensation of liver cirrhosis, the results of a 3-month survival period in terms of treatment and immediate decision-making related to liver transplantation will be relevant.
As can be seen from Table 2, in patients at the stages of subcompensation and decompensation, having up to 10 and 11-19 points on the MELD scale, the 3-month survival rate is very high and amounts to 98,1% and 94,0%, respectively. With an increase in the MELD score, the three-month survival of patients decreases. In patients with 30-39 or more than 40 points, the prognostic three-month survival rate decreases sharply.
Thus, the results of the study of serological, virological and clinical-biochemical data in patients with cirrhosis of the liver in the outcome of chronic viral hepatitis C, with high values on the MELD scale, are recommended for timely hospitalization or surgical intervention. Taking into account the polysymptomicity of the clinical characteristics of liver cirrhosis in the outcome of HCV, it is promising to identify the leading syndrome, followed by its concretization and definition of therapeutic tactics.
Conclusions
The average score on the MELD scale in the analyzed patients significantly increased with an increase in the severity of cirrhosis in the outcome of HCV: in patients with subcompensated stage of liver cirrhosis, the index was 15± 1,66, and with decompensated stage of class C disease on the Child-Pugh scale – 25± 0,8 (p<0.001). Statistically significant correlation was also noted by the indicator of the MELD scale and the levels of albumin (r = -0,69), γ-globulin (r = 0,73) and AFP (r = 0,59).
Библиографическая ссылка
Ташполотова А.Ш., Суранбаева Г.С., Алишерова А.Ш., Анарбаева Ж.А., Мурзакулова А.Б., Заирова И.Т., Шолпанбай Уулу М.Н. APPLICATION OF THE MELD SCALE TO ASSESS THE SEVERITY OF LIVER CIRRHOSIS IN THE OUTCOME OF CHRONIC HEPATITIS C IN THE KYRGYZ REPUBLIC // European Journal of Natural History. 2022. № 6. ;URL: https://world-science.ru/en/article/view?id=34297 (дата обращения: 28.07.2026).
DOI: https://doi.org/10.17513/ejnh.34297