
Scientific journal
European Journal of Natural History
ISSN 2073-4972
ИФ РИНЦ = 0.204
IMMUNOPHENOTYPING AND FREQUENCY THE PREVALENCE AMONG PATIENTS CHILDREN ACUTE LYMPHOBLASTIC LEUKEMIA

Currently, disease acute leukemia worries of all, occurs and in developing and in developed countries, and is detected in people of all races, and among the adult population, so and among children’s age.
Acute leukemia – is acute malignant disease of the blood system, with defeats at the level of deterministic genus-parent stem cells or early cellular predecessor, characterized by the availability of blast cells in the bone marrow puncture or in peripheral blood from 20 % and more.
As noted by the authors [4], when making a diagnosis of acute leukemia, cytogenetic, cytochemical, morphological studies remain a powerful tool in clinical practice, but for a detailed study of bone marrow cells, by method flowing cytofluorimetry and at the correct collection material, undoubtedly have great advantages.
In justification of immunophenotype diagnosis using the method of flow cytofluorimetry in acute leukemiaб it is necessary to appreciate the features of the immunophenotype characteristics oftumor cells and determine the directionality of B and T, and exclude myeloid and rare variants of unclear linearity.
Well- known, and today, relate to B-cell markers at the B-lymphoblastic leukemia CD19, CD79a (cyCD79a). CD22 (cyCD22), CD10, CD20. But the phenotypes of CD19+, CD10+ in acute B-lymphoblastic leukemia is the most prevalent. And this variant of leukemia called “common”.
In acute lymphoblastic leukemia (T-lymphoblastic leukemia/lymphoma), tumor cells have a phenotype similar with T-linear predecessor. By early markers at T-ALL relate CD99, CD34, CD1a, TdT (Terminal deoxynucleotidyl Transferase), cyCD3, CD7.
For diagnosis, it is first necessary to take into account and appreciate cytoplasmic expression of CD3, which is the only linear-specific antigen of the T-line.
For determine the linear affiliation of tumor cells, antibody kits are used, on the recommended by the Euroflow Consortium [8], the European Leukemia Network [6], the international consensus Bethesda [9], and also used for differential diagnosis classification the EGIL [5] and classification the World Health Organization (WHO) [7].
At staging a diagnosis and determining the variant of tumor cell linearity, us clinicians need to make the right choice of polychemotherapy.
For targeted treatment of the oncohematological diseases in patients children and adults, and for achieve a good result from the performed polychemotherapy (PChT), it is necessary to spend out immunophenotyping on system HLA-main complex histocompatibility.
Spending a closely related, unrelated bone marrow transplantation lets at the availability of healthy HLA-identical donor [2; 3] or placental blood [1]. Transplantation hematopoietic stem cells bone marrow gives the best results for increased survival in the treatment of oncohematologic diseases.
The aim of our study is to determine frequency the prevalence and early diagnosis analysis of the immunophenotype of tumor cell linearity at acute lymphoblastic leukemia in patients children of the Kyrgyz Republic(Kirgizia).
Materials and research methods
The research group from November 2016 to December 2018 have entered with acute lymphoblastic leukemia – 70 patients of children (female – 25, male – 45), all citizens of the Kyrgyz Republic (Kirgizia), at the age of 1,5 years to 16 years, of them kirgiz nationality – 52 (female – 22, male – 30), and residents of the Russian-speaking population of the Kyrgyz Republic(mixed nation and different nationalities) – 18 patients of children (female – 3, male – 15) who were undergoing research in the department of pediatric oncology of the National Center for Oncology and Hematology of the Ministry of Health of the Kyrgyz Republic (Kirgizia) and in the Department of Pediatric Hematology of the Osh Interregional Clinical Children’s Hospital in Osh, in St. Petersburg consulted doctors hematologists Eurasian Center of Oncohematology, Immunology and Therapy.
Method immunophenotyping by dint of flowing cytofluorimetry conducted the first time and research was conducted in city Bishkek Kyrgyz Republic (Kirgizia) [4].
Method by dint of flowing cytofluorimetry
The material for the study is the bone marrow. Patients made puncture of the sternum. For obtain a qualitative authentic result, the obtained analysis should not be with impurity blood and not destroyed the cells during the test-sample preparation to immunophenotyping. Immunophenotyping of leukemia (blast) cells performed on a flow cytofluometer Cytomics FC500 (Beckman Coulter, USA) using monoclonal antibodies Beckman Coulter.
Statistical processing of the results included the analysis of standard criteria X2-square, which was used to assess the significance of differences in the occurrence of certain characteristics between the control group and the test group. Determination of the “p”, the corresponding value found. X2-square performed considering one degree of freedom.
All mathematical calculations and statistical analysis of the overall study was performed using a personal computer using the package application programs for spreadsheets – Microsoft – Excel M version 7.0, for Windows 95, for Windows-based 2010, Statistica-5.
Research results and discussion
During our research, the diagnosis of acute lymphoblastic leukemia was established on the basis of common clinical data and complex laboratory-diagnostic indicators.
Comparative characteristics of the frequency of occurrence of immunophenotype variants B-ALL and T-ALL in the Kyrgyz Republic (on the classification of the European group of the immunological characteristics of acute leukemia/EGIL) [5]
|
В-ALL п = 58 |
Т-ALL п = 12 |
||
|
pro В-ALL(ВI) |
5 % |
pro Т-ALL(ТI) |
0 % |
|
В-common (BII)* |
91 % |
pre Т-ALL(ТII)* |
67 % |
|
pre В-ALL (ВIII) |
0 % |
cortical (ТIII) |
25 % |
|
В-ALL(BIV) |
4 % |
T-ALL(ТIV) |
8 % |
Note: *p < 0,001.
As can be seen from the presented table, in the Kyrgyz Republic (Kirgizia) on the frequency prevalence is found B-ALL: B-ALL (BI) in 5 % of cases, B-common (BII) in 91 % of cases, pre-B-ALL (BIII) in 0 % of cases, B-ALL (BIV) in 4 % of cases and T-ALL: pro T-ALL (TI) in 0 % of cases, pre-T-ALL (TII) in 67 % of cases, cortical (TIII) in 25 % of cases, T-ALL (TIV) in 8 % of cases. In terms of significance, B-common (BII) and pre-T-ALL (TII) have statistically highly significant differences, where p < 0.001.
As be seen from Fig. 1, the prevalence of acute lymphoblastic leukemia in the Kyrgyz Republic (Kirgizia) is the prevalence among patient’s children in 83 % of cases of B-lymphoblastic leukemia/ lymphoma(B-ALL/lymphoma) and T-lymphoblastic leukemia/lymphoma(T-ALL/lymphoma) in 17 % of cases.
According to the data presented in Fig. 2, T-lymphoblastic leukemia/lymphoma is detected among patient’s female children in 12 % of cases and B-lymphoblastic leukemia/lymphoma in 88 % of cases, and in patient’s male children T-lymphoblastic leukemia/lymphoma in 20 % of cases and 80 % of cases of B- lymphoblastic leukemia/lymphoma. B-lymphoblastic leukemia/lymphoma a most prevalence and among patients children male and female.
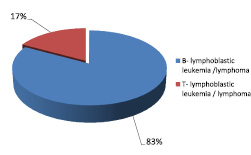
Fig. 1. The prevalence in the Kyrgyz Republic among children of acute lymphoblastic leukemia B-lymphoblastic leukemia/lymphoma(B-ALL/lymphoma)and T-lymphoblastic leukemia/lymphoma (T-ALL/lymphoma)
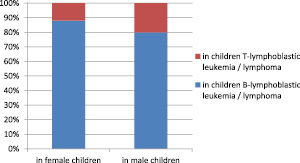
Fig. 2. Prevalence of acute lymphoblastic leukemia B-lymphoblastic leukemia/lymphoma and T-lymphoblastic leukemia/lymphoma among patients children female and male in the Kyrgyz Republic(Kirgizia)
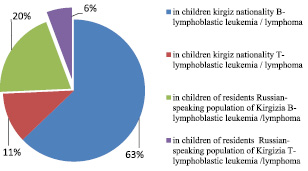
Fig. 3. Comparative characteristics frequency of the prevalence of B-ALL/lymphoma and T-ALL/lymphoma among children of kirgiz nationality and residents of the Russian-speaking population of the Kyrgyz Republic (Kirgizia)
As be seen from Fig. 3, the prevalence of T-lymphoblastic leukemia/lymphoma among patient’s children of kirgiz nationality in 11 % of cases and in 63 % of cases of B-lymphoblastic leukemia/lymphoma, and among patients children residents of the Russian-speaking population of the Kyrgyz Republic(mixed nation and different nationalities Kirgizia)- in 6 % of T-lymphoblastic leukemia/lymphoma and B-lymphoblastic leukemia/lymphoma in 20 % of cases.
According to the results of Figure 4, detected in patients children kirgiz nationality among female of B-ALL/lymphoma in 33 % and among patients male in 67 % of cases and T-ALL/ lymphoma among female in 13 % of cases and among male in 87 % of cases. And among patients children residents of the Russian-speaking population of the Kyrgyz Republic (Kirgizia) B-ALL/ lymphoma in female children in 6 % and among children male in 94 % of cases and T-ALL/ lymphoma among children female in 12 % of cases and among children male in 88 % of cases.

Fig. 4. Frequency the prevalence of acute lymphoblastic leukemia among children of kirgiz nationality and residents of the Russian-speaking population of the Kyrgyz Republic (Kirgizia)
Thus, on the frequency of prevalence among patients children in the Kyrgyz Republic(Kirgizia) with acute lymphoblastic leukemia is more often detected B-lymphoblastic leukemia/lymphoma on the compared with T-lymphoblastic leukemia/lymphoma.
In acute lymphoblastic leukemia (B-lymphoblastic leukemia/lymphoma and T-lymphoblastic leukemia/lymphoma), in the main targeted process using flowing cytofluorimetry to establish the B and T linear direction of tumor cells.
For elicitation the features of the course and frequency of the prevalence of acute leukemia among patients children in the Kyrgyz Republic(Kirgizia), is necessary further research, which makes it possible for the timely selection of therapy and targeted treatment when planning an unrelated, closely related bone marrow transplant.
Conclusion
1. Research bone marrow in patient’s children with acute lymphoblastic leukemia method by dint of flowing cytofluorimetry.
2. Screening study for determine the linear directing of tumor cells.
3. Identify immunological variant of acute lymphoblastic leukemia.
4. Immunophenotyping by dint of flowing cytofluorimetry makes it possible to elicitation the characteristic T and B linear immunophenotype of tumor cell and timely selects effective program chemotherapy.
Библиографическая ссылка
Baratova D.А., Mamatysaeva U.A. IMMUNOPHENOTYPING AND FREQUENCY THE PREVALENCE AMONG PATIENTS CHILDREN ACUTE LYMPHOBLASTIC LEUKEMIA // European Journal of Natural History. 2019. № 2. ;URL: https://world-science.ru/en/article/view?id=33965 (дата обращения: 29.07.2026).