
Scientific journal
European Journal of Natural History
ISSN 2073-4972
ИФ РИНЦ = 0.204
PROVISION OF FREE SPECIALIZED SURGICAL CARE IN A SANATORIUM FOR RESTORATION OF KAZAKHSTAN WOMEN’S FERTILITY

In the late 20th century, there was a significant emigration of population (15-20 %) from Kazakhstan, including qualified medical workers. The government of Kazakhstan has taken a few legislative acts to overcome the undesirable tendencies associated with the deterioration in the level of medical care. The protection of reproductive health, maternal and child health, the improvement of the quality of life of women, as well as the guaranteed volume of free medical care (GVFMC) in the Republic of Kazakhstan are guaranteed by legislative acts [1,2]. GVFMC is granted to citizens of Kazakhstan and immigrants (oralmans) at the expense of budgetary funds [1], and includes preventive, diagnostic and therapeutic medical services which have the greatest proven effectiveness [3]. As a rule, recovery treatment and medical rehabilitation of patients are conducted in sanatorium-resort organizations [4-7]. Starting from 2015, at the Sanatorium “Okzhetpes” “Almaty” for the first time in Kazakhstan, minimally invasive surgical methods such as hysteroscopy, hysteroscopy, laparoscopy, vaginal surgery, cystourethropexy were introduced into the medical practice of the sanatorium clinic.
The aim of this work is to study the effectiveness of experimental introduction by gynecological service into medical practice of the clinic of the sanatorium “Okzhetpes” “Almaty” of free specialized and high-tech medical care with the use of endovideosurgery and their influence on restoration of women’s fertility.
Clinical techniques of treatment in the sanatorium-resort organization
Sanatorium “Okzhetpes” “Almaty” in Almaty is a modern multi-functional sanatorium and resort complex, which provides high-quality medical services by doctors in 26 specialties [4], comfortable rest, as well as therapeutic rehabilitation using natural, climatic and other factors in 13 different profiles, including diseases oe-mail: f circulatory, nervous, musculoskeletal and genitourinary systems, respiratory, digestive, nutrition disorders, metabolic disorders, etc.
Patients from Kazakhstan, Russia, Canada, Kyrgyzstan, Latvia, Uzbekistan, Tajikistan and other countries note the effect of the treatment and improvement of the subjective evaluation of life quality [5]. This contributes to the development of medical tourism [7,8]. However, the cost of the voucher, including payment for 4 meals a day, accommodation and reception of physiotherapy procedures up to 40 titles, is 25000 tenge ($ 80, December 2015) per day and is not always available. As is known [9], rural population, especially non-working women, often faces many obstacles to access to high-tech medical services (HTMS) and long waiting for the necessary medical care [10,11]. Specialized medical care (SMC) is 70000 tenge ($220) for the operation of hysteroscopy, 107000 tenge ($340) for the operation of laparoscopy and 600000 tenge ($1900) for highly specialized medical care operation. In this relation, sanatorium “Okzhetpes” “Almaty” has significantly expanded the list of free medical services within GVFMC [12]. As an experiment, such minimally invasive methods of surgical treatment as hysteroscopy, hysteroresectoscopy, laparoscopy, vaginal surgery, cystourethropexy, were firstly introduced in the medical practice of sanatorium clinic.
The main tasks of the gynecological service of the clinical diagnostic center of sanatorium “Okzhetpes” “Almaty” are introduction of advanced technologies in the field of gynecology, the provision of specialized and high-tech medical care in diagnosis and treatment of gynecological diseases with the use of endovideosurgery [12, 13]. Since 2015, the gynecological service is a participant in the republican program for the provision of SMC to the public in framework of the state order. The solution of these tasks is carried out by the employees of the Department of Obstetrics and Gynecology No.1 of Asfendiyarov KazNMU.
Materials and methods of research
For 2015-2016, 83 patients with various gynecological pathologies were treated. The operating unit is equipped with a laparoscopic technical kit from Karl Storz. Several types of gynecological operations are performed by laparoscopic (Fig. 1, a) and vaginal accesses, as well as intrauterine surgery using a hysteroscope and a hysteroresectoscope (Fig. 1, b).
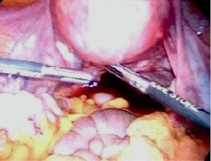

(a) (b)
Fig. 1. Surgical operation laparoscopy (a) and hysteroscopy (b) in the clinic of Sanatorium “Ok-Zhetpes” “Almaty”
In this work the clinical, analytical and statistical methods of investigation were used. The analysis of the case histories was carried out, the somatic and reproductive history, the structure of the performed gynecological operations and their outcomes are studied.
All procedures performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration. No animal or human studies were carried out by the authors for this article. Data are anonymous and will be used for research purposes.
Analysis revealed that 77 (92.8 %) of the 83 hospitalized patients are residents of Almaty, 5 patients (6.0 %) are residents of Almaty and Zhambyl regions, 1 (1.2 %) is from Astana. Patients from Almaty were hospitalized in the direction of polyclinic of the city hospital No. 5 – 47 (56.6 %) hospitalizations, the city polyclinic CP No.12 – 10 (12 %) hospitalizations; CP No 4 – 6 (7.2 %); CP No. 3, 15 and 17 – 5 (6.0 %); CP No. 6, 11, 16, 21 – 4 (4,8 %).
Analysis of social indicators revealed that housewives were 46 (55.4 %), retirement age – 6 (7.2 %), working women – 31 (37.4 %). The ethnic composition was studied: Kazakhs – 76 (91 %), Russians – 3 (4 %), Uighurs – 3 (4 %), Korean – 1 (1.2 %). The age of women ranged from 18 to 70 years. The number of women of active reproductive age was 45 (54.2 %), late reproductive age – 22 (26.5 %), in perimenopause, postmenopause – 16 (19.3 %).
The average length of stay of patients in the gynecological department for 2015 – 2016 was 5.0 ± 0.5 bed-days.
Results of the research and their discussion
The structure of the indications for hospitalization of patients in the gynecology department is shown in Fig. 2. For 2015-2016 years, 83 patients were hospitalized on the state order and 93 gynecological operations were performed. 10 (12.0 %) of 83 patients underwent simultaneous operations (hysteroscopy and laparoscopy). Table 1 shows the structure of diseases of patients by year – in 2015 and 2016. 40 of 83 patients have previous long-term infertility. Every fifth patient was hospitalized with a diagnosis of infertility of mixed genesis, each tenth – with tubal-peritoneal infertility. The second place is occupied by benign neoplasms of the ovaries, including endometriosis cysts. Among the hysteroscopic operations, the operations of endometrial and cervical polypectomy, endometrial biopsy prevail. All of them were accompanied by fractional diagnostic scraping of the uterine cavity and cervical canal. In addition to specialized medical care (SMC), the sanatorium provides high-tech medical services (HTMS) concerning uterine prolapse and stress incontinence (Table 1).
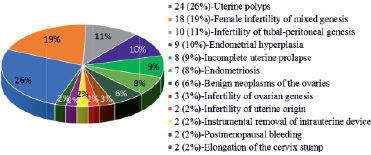
Fig. 2. Structure of diseases of hospitalized patients
Table 1
Statistics and the number of patients treated in 2015-2016 on nosologies
|
Type MC |
Nosology ICD-10 |
2015 |
2016 |
||
|
Quantity |
% |
Quantity |
% |
||
|
SMC |
Female infertility of mixed genesis |
11 |
20.4 |
7 |
17.9 |
|
Infertility of tubal-peritoneal genesis |
6 |
11.1 |
4 |
10.3 |
|
|
Endometriosis (infertility) |
4 |
7.4 |
3 |
7.7 |
|
|
Benign neoplasms of the ovaries |
4 |
7.4 |
2 |
5.1 |
|
|
Infertility of ovarian genesis |
2 |
3.7 |
1 |
2.6 |
|
|
Infertility of uterine origin |
2 |
3.7 |
– |
– |
|
|
Endometrial hyperplasia |
2 |
3.7 |
7 |
17.9 |
|
|
Uterine polyps |
13 |
24.1 |
11 |
28.2 |
|
|
Postmenopausal bleeding |
– |
– |
2 |
5.1 |
|
|
Instrumental removal of intrauterine device |
2 |
3.7 |
– |
– |
|
|
HTMS |
Uterine prolapse |
7 |
12.9 |
1 |
2.6 |
|
Extirpation of cervix stump, hysterectomy |
1 |
1.9 |
1 |
2.6 |
|
|
Total surgical procedures |
54 |
100 |
39 |
100 |
|
The analysis of the surgical treatment for 2015-2016 has revealed that operations were performed laparoscopically in 25 (26.9 %) cases, in 58 (62.4 %) – hysteroscopically and in 10 (10.7 %) – by vaginal access. The structure of gynecological operations was as follows: in 2015, 54 surgical procedures to 51 patients were made, in 2016 – 39 manipulations to 32 patients. Table 2 shows the types and number of intrauterine manipulations for 2015-2016.
In the structure of laparoscopic operations (Table 3), the leading steels of cystectomy (10 operations) and salpingo-ovariolysis (7 operations).
In 2015, more operative interventions were performed by vaginal access (in the framework of HTMS): anterior and posterior colpotomy, colporrhaphy with bladder transposition, Kelly’s cystourethropexy – 8 operations, hysterectomy without appendages – 1, extirpation of the cervix stump – 1.
Table 2
Structure of intrauterine manipulation for 2015-2016
|
Types of intrauterine manipulation |
2015 |
2016 |
||
|
Quantity |
% |
Quantity |
% |
|
|
Diagnostic hysteroscopy |
5 |
13.8 |
3 |
13.6 |
|
Polypectomy |
13 |
36.1 |
9 |
40.9 |
|
Scraping the uterine cavity |
13 |
36.1 |
9 |
40.9 |
|
Removal of the intrauterine device |
2 |
5.6 |
– |
– |
|
Dissection of synechia (hysteroresectoscopy) |
1 |
2.8 |
1 |
4.6 |
|
Uterine septum dissection (hysteroresectoscopy) |
2 |
5.6 |
– |
– |
|
Total: |
36 |
100 |
22 |
100 |
Table 3
Structure of laparoscopic operations for 2015-2016
|
Types of laparoscopic operations |
2015 |
2016 |
||
|
Quantity |
% |
Quantity |
% |
|
|
Salpingo-ovariolysis, adhesiolysis |
2 |
14.3 |
5 |
45.4 |
|
Cystectomy |
6 |
42.9 |
4 |
36.4 |
|
Fimbrioplasty |
– |
1 |
9.1 |
|
|
Ovarian drilling |
2 |
14.3 |
1 |
9.1 |
|
Adnexectomy |
1 |
7.1 |
– |
|
|
Myomectomy |
3 |
21.4 |
– |
|
|
Total: |
14 |
100 |
11 |
100 |
The results of treatment of patients with various gynecological pathologies are characterized by the absence of relapses of genital prolapse, benign neoplasms of the ovaries and the uterus, and the absence of complications in the postoperative period.
The experimental introduction and expansion of the list of free medical services within the framework of GVFMC into the medical practice of sanatorium allowed “Okzhetpes” “Almaty” JSC to provide surgical assistance to socially vulnerable segments of the female population with impaired reproductive function, as well as to significantly shorten the period of their rehabilitation and improve the outcomes of surgical treatment. Long-term results indicate early restoration of fertility after surgical treatment in 8 (20.0 %) of 40 patients with previous long-term infertility: in 6 (15 %) patients the pregnancy ended by vaginal parturition; in 1 (2.5 %) – by a planning cesarean section, and 1 (2.5 %) is now in pregnant.
Women from socially vulnerable segments of the population note an improvement in the subjective evaluation of the quality of life as a special effect of the treatment received in the highly comfortable conditions of the sanatorium.
Conclusion
The experimental introduction of hysteroscopy, hysterosectoscopy, laparoscopy and vaginal surgery in comfortable sanatorium allowed to significantly shorten the rehabilitation period, contributed to the early restoration of fertility and the onset of pregnancy in 20 % of patients with previous long infertility caused by infertility of mixed genesis, infertility of tubal-peritoneal genesis, endometriosis, infertility of ovarian genesis, infertility of uterine origin. Women from socially vulnerable segments of population note an improvement in subjective evaluation of life quality. The results obtained allow projecting this experience on similar medical institutions of sanatorium-resort type.
Authors are grateful to Amanzholova B.K. for the discussion of the manuscript, to Shaimardanova L.K. and other doctors for assistance in referring patients to the clinic.
The authors declare no conflict of interest.
This research received no specific grant from any funding agency in the public, commercial, or from non-profit sectors.
Библиографическая ссылка
Omarova G.K., Khassenova M.D., Rakhimzhanova A.Kh., Orazkulov M.O. PROVISION OF FREE SPECIALIZED SURGICAL CARE IN A SANATORIUM FOR RESTORATION OF KAZAKHSTAN WOMEN’S FERTILITY // European Journal of Natural History. 2019. № 1. ;URL: https://world-science.ru/en/article/view?id=33949 (дата обращения: 13.07.2026).