
Scientific journal
European Journal of Natural History
ISSN 2073-4972
ИФ РИНЦ = 0.204
INFLUENCE ON QUALITY OF LIFE OF MANUAL THERAPY’S METHODS ON PREGNANT WOMEN DIAGNOSED WITH DORSOPATHY

The relevance of dorsopathy problem essentially lays in the morphological multiplicity of the forms included in this collective concept as well as in the high prevalence among the population [2, 7]. According to WHO experts at the present time in developed countries the problem of back pain can be compared to the pandemic and is a serious medical and socio-economic problem [9]. During lifetime, at least one episode of back pain occurs for 70-80 % of the population, where the annual rate varies from 25 % to 60 % in different ethnic groups [4, 1, 6, 14]. For preagnent women pain in the lower back and pelvic pain both caused by dorsopathy are the most common phenomenons, and have recently been considered as a normal part of pregnancy [6]. In the national literature there is little data on the occurrence of dorsopathy for pregnant women and its possible methods of treatment [13]. As return, dorsopathy leads to a painful predominantly syndrome in the back area, interferes with daily actions, it also affects the emotional state (leads to depression), a decrease in sexual activity, and there is a disturbance in sleep [6]. Various foreign studies have shown that about 50 % of pregnant women experience back pain at different stages of their pregnancy. For 25 % of pregnant women back pains leads to serious health problems with some half disabling already at first and second trimesters, and for 8 % leads to disabilities of varying severity [10]. In addition, often symptoms of dorsopathy are taken as the symptoms for termination of pregnancy at different gestational periods, so it is necessary to study deeply this problem in order to reduce hospitalizations themselves as well as the aimlessly practice of magnesia and tocolytic therapy for pregnant women. During pregnancy the load on the lumbosacral spine increases, especially at the very peak of fetal growth 16-18 weeks, 26-28 weeks, 32-34 weeks [12]. It should be noted that the health of women, mothers and children is the main and objective indicator of the health of the population and therefore the protection of women’s health is one of the priorities of the state [11].
Goal of the research is to improve the quality of life of pregnant women with dorsopathies using the methods of manual therapy (MT).
Materials and methods of research
The study defining possible effect of MT methods on the quality of life of a pregnant woman with dorsopathy. During this period, 50 pregnant women were examined (gestation period – II and III trimester (from 18 to 38 weeks of pregnancy) with a diagnosis of “dorsopathy”, among which two groups were identified (control (n = 25) and study(n = 25)). The age of the pregnant women participating in this study was from 22 to 39. Before the application of MT methods on pregnant women, the functional condition of the pelvic girdle was assessed. This approach made it possible to determine the necessity of applying methodical techniques of a mixed character, i.e. related, both to the upper and lower parts. In the standing position were evaluated the following parameters: the direction of the pelvic plane, the descent of any margin, the curvature of the spine, the tension of certain muscle groups, the state of the pelvic lobes, the lower edge of the gluteal muscles, the condition of the thighs, legs and feet, and the lengths of the lower extremities. During the assessment of the functional state of the pelvis the position of the knee joints, as well as the size of the arch of the foot are important. A particularly significant effect on the pelvis is the unilateral overextension of the knee joint. In addition was performed an evaluation of the Michaelis rhombus and the condition of the interannual and anal folds [5]. As the next step while applying the MT the following methods were used: 1) diagnosis and correction of dysfunction of the thoraco-abdominal diaphragm; 2) decompression at the level of the lumbar spine, balancing the chest lumbar fascia, lumbar and quadrate muscles; 3) correction of lumbosacral articulation L5S; 4) correction of the sacroiliac joint; 5) diagnosis and correction of dysfunction of the false joint; 6) diagnosis and correction of coccyx dysfunction; 7) diagnosis and correction of dysfunction of the pelvic muscles. An assessment of the quality of life of pregnant women with dorsopathies was conducted using the following methords: EuroQol-5D questionnaire, the Oswestry questionnaire, the medical and social characteristics, the pain syndrome using the McGill questionnaire, the visual analogue scale (VAS), and the verbal evaluation score scale [2, 8].
Results of research and their discussion
Preliminary results of the current study have been already obtained and were evalueted using different methods, assessing the condition of preagnatn women before and after applying MT. Were analyzed the following paramenters of pregnant women condition: sleep, pain/discomfort, anxiety/ depression and self-care.
According to the verbal assessment scale [3, 15] there was as well a decrease in the pain syndrome. Six pain assessment options were taken into account: 0 no pain, 2 weak pain, 4 moderate pain, 6 severe pain, 8 very severe pain, 10 unbearable pain. Prior to the MT pregnant women were asked to assess their current pain stage and gave the following numbers : “4” was noted for 8 women (32 %), “6” – for 5 (25 %), “8” – for 12 (48 %) and no one voted for the following levels: “0”, “2” and “10” – (0 %) (Fig. 1).
After applying the MT methods pregnant women were again asked to assess their condition and the results were the following: “0” was noted for 10 of them (40 %), “2” – for 15 (60 %) and “4”, “6”, “8” and “10” – 0 (0 %) (Fig. 2).
Table 1
The indicator of quality of life – sleep
|
Oswestry’s questionnaire [3,15]: |
Before MT ( %) |
After MT ( %) |
|
(1) I sleep good and the pain does not violate it |
5 (20 %) |
21 (84 %) |
|
(2) I can sleep soundly only with the help of pills |
12 (48 %) |
4 (16 %) |
|
(3) Even after taking the pill, I sleep less than 6 hours at night |
2 (8 %) |
0 (0 %) |
|
(4) Even after taking the pill, I sleep less than 4 hours at night |
2 (8 %) |
0 (0 %) |
|
(5) Even after taking the pill, I sleep less than 2 hours at night |
0 (0 %) |
0 (0 %) |
|
(6) I do not sleep at all due to pain |
1 (4 %) |
0 (0 %) |
Table 2
The indicator of quality of life – pain and discomfort
|
EuroQol-5D questionnaire [3,8]: |
Before MT ( %) |
After MT ( %) |
|
“I do not feel pain or discomfort” |
4 % (n = 1) |
24 (96 %) |
|
“I experience mild pain or discomfort” |
72 % (n = 18) |
1 (4 %) |
|
“I’m completely bedridden” |
24 % (n = 6) |
0 (0 %) |
|
Oswestry’s questionnaire [3,15]: |
||
|
(1) Currently I have no pain |
0 (0 %) |
20 (80 %) |
|
(2) Currently the pain is very easy |
8 (32 %) |
5 (20 %) |
|
(3) Currently moderate pain |
13 (52 %) |
0 (0 %) |
|
(4) At the present time the pain is very strong |
2 (8 %) |
0 (0 %) |
|
(5) At the moment the pain is very strong |
2 (8 %) |
0 (0 %) |
|
(6) At the present time the pain is so strong that it is difficult to imagine |
0 (0 %) |
0 (0 %) |
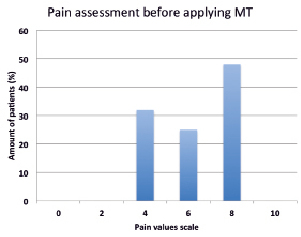
Fig. 1. Assessment of the pain syndrome of pregnant women with dorsopathy using a verbal evaluation scale before applying manual therapy
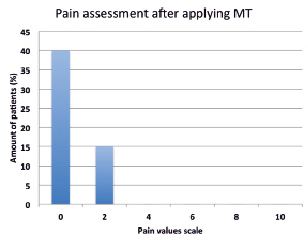
Fig. 2. Assessment of the pain syndrome of pregnant women with dorsopathy using a verbal evaluation scale after applying manual therapy
Table 3
The indicator of quality of life – anxiety and depression
|
EuroQol-5D questionnaire [3, 8]: |
Before MT ( %) |
After MT ( %) |
|
“I do not experience anxiety or depression” |
9 (36 %) |
25 (100 %) |
|
“I experience mild anxiety or depression” |
13 (52 %) |
0 (0 %) |
|
“I experience extreme pain or discomfort” |
3(12 %) |
0 (0 %) |
Table 4
The indicator of quality of life – sdelf-care
|
EuroQol-5D questionnaire [3, 8]: |
Before MT ( %) |
After MT ( %) |
|
“I have no problems with maintenance” |
6 (24 %) |
24 (96 %) |
|
“I have some problems with washing or dressing” |
18 (72 %) |
1 (4 %) |
|
“I’m completely bedridden” |
1 (4 %) |
0 (0 %) |
|
Oswestry’s questionnaire [3, 15]: |
||
|
(1) Self-service is intact and does not cause additional pain |
3 (12 %) |
16 (64 %) |
|
(2) Self-service is intact, but causes additional pain |
9 (36 %) |
9 (36 %) |
|
(3) In self – care due to increasing pain I act slowly |
8 (32 %) |
0 (0 %) |
|
(4) In self-service, I need some help, but most of the actions I do myself |
3 (12 %) |
0 (0 %) |
|
(5) I need help with most self-service activities |
2 (8 %) |
0 (0 %) |
|
(6) I can not get dressed, I wash with great difficulty and I stay in bed |
0 (0 %) |
0 (0 %) |
Conclusion
In the following study, the results that have been obtained allow us to speak about the effectiveness of manual therapy’s use on pregnant women at the II and III trimester of pregnency with the results of not only reducing but also completely eliminating the pain syndrome caused by dorsopathies in most of the cases. In the study group there was a marked improvement immediately after the first session of manual therapy. Another preliminary results of the study is that an analysis of the outcome of pregnancies showed a decrease in the number of abdominal delivery, which is fundamental in light of current attitudes toward reducing the rate of cesarean section (87.5 % of women were delivered through natural birth canals). It should be noted that all children (from women from the study group) were born in a satisfactory state with an Apgar score of 7 or more. A decrease in the number of sick leave cards for this disease was noted, as well as an improvement in the quality of life for pregnant women. The obtained data confirm the effectiveness and necessity of sending pregnant women with dorsopathies in the II and III trimesters to manual therapists for appropriate treatment.
Библиографическая ссылка
Vaganova Y.A., Suslova G.A., Gaidukov S.N. INFLUENCE ON QUALITY OF LIFE OF MANUAL THERAPY’S METHODS ON PREGNANT WOMEN DIAGNOSED WITH DORSOPATHY // European Journal of Natural History. 2018. № 2. ;URL: https://world-science.ru/en/article/view?id=33855 (дата обращения: 15.07.2026).