

Liver diseases caused by hepatotropic viruses are currently an urgent medical and social problem of infectology. Modern research methods have shown that the etiology of infectious diseases of the liver is not limited to “hepatitis viruses”. Hepatitis can also be caused by herpes viruses (herpes simplex virus, Epstein-Barr virus, cytomegalovirus, human herpes virus types 6 and 7, etc.), which also have hepatotropy, but do not belong to “hepatitis viruses”. The prevalence of viral hepatitis, including herpesvirus infections, has reached a critical level worldwide in recent years and, unfortunately, continues to grow. [1,2,3]. According to WHO data from 1987, more than 90% of the world’s population is infected with herpes infection. The etiology, clinical and laboratory diagnostics, treatment and prevention of viral hepatitis have not yet been sufficiently studied. The spectrum of herpes-induced liver lesions is quite wide: from asymptomatic hepatitis to fulminant forms [4,5,6,7]. For example, HSV-hepatitis is characterized by a severe course and often occurs in a fulminant form with the development of signs of acute liver failure and encephalopathy. Mortality according to different authors is high and ranges from 40% to 80% [4,5,6,7]. Therefore, despite significant progress in our knowledge of viral hepatitis, their etiology, pathogenesis, clinic, laboratory diagnostics, treatment and prevention, it is necessary to continue studying this urgent problem.
Purpose of the study: to compare clinical and laboratory characteristics of acute viral hepatitis B (HBV) and unverified hepatitis in individuals infected with herpes simplex virus (HSV).
Materials and methods of research
A retrospective comparative analysis of clinical and laboratory data of 65 patients was carried out (with acute viral hepatitis – 45 patients and unverified hepatitis infected with the herpes simplex virus – 20 patients who were hospitalized at the Republican Clinical Infectious Diseases Hospital in Bishkek for the period 2018-2020.
Results of the research and discussions
Among the studied patients with viral hepatitis was: HBV – 45 patients, with unverified hepatitis – 20. HBV was registered in 28 men (62%) and 17 women (38%), and in the group of patients with unverified hepatitis, women were more often ill – 12 (60%) cases, men were 8 (40%), as can be seen in Fig.1.
Acute viral hepatitis B was most often registered in people aged 19-29 years (60%), in the age group of 30-39 years the rate decreased almost three times (24.4%). Beginning at age 40 and older, HBV dropped significantly to 6.7%.
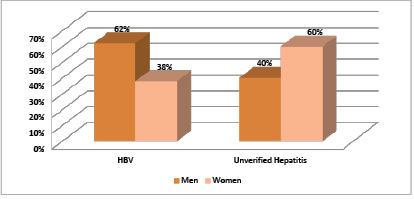
Fig. 1. Gender ratio of men and women with HBV and unverified hepatitis
Unverified hepatitis was more common in young people aged 19-39 years (35-20%), starting from the age of 50, the incidence of unverified hepatitis increased markedly to 30%.
When studying the epidemiological anamnesis, it was found that among patients with HBV, 13 people (29%) had contact with blood during dental treatment, 5 (11%) – during surgical operations, 4 (10%) – through manicure and tattoos, 2 (4 %) – with intravenous and intramuscular injections, 2 (4%) – with blood transfusion, 1 patient (2%) with the use of other people’s razors, in 17 (40%) patients it was not possible to find out the source of infection.
The source of infection in unverified hepatitis has been established: 4 (20%) cases during dental treatment, 1 (5%) patient was infected through a manicure, and in the remaining 15 (75%) cases the source of infection is unknown.
More than 55% of cases of HBV and unverified hepatitis proceeded in a moderate form.
Severe forms were observed more with unverified hepatitis, which amounted to 35%, and with HBV – only 26.7%. Two cases with an extremely severe form with unverified hepatitis (10%) and one case with HBV (2.2%) with a fatal outcome, unfortunately, have been reported.
Studying the nature of the onset of the disease, it turned out that the acute onset of the disease is characteristic of unverified hepatitis – 70%, while the gradual onset of the disease was characteristic of patients with HBV – 55.6%, the acute onset of the disease was recorded in 44.4% of cases of HBV.
In both compared groups, patients were more often hospitalized on the 7-10th day from the onset of the disease, which, apparently, was associated with the onset of the icteric period.
Clinical picture of HBV and unverified hepatitis
|
Clinical manifestations |
ABHV (45) |
Unverified Hepatitis (20) |
|
Fever |
46,7% |
85,0% |
|
Sleep disturbance |
13,3% |
30,0% |
|
Asthenic syndrome |
95,5% |
95,0% |
|
Catarrhal syndrome |
4,0% |
25,0% |
|
Dyspeptic syndrome |
71,1% |
80,0% |
|
Pain syndrome |
100,0% |
100,0% |
|
Arthralgic syndrome |
24,4% |
25,0% |
|
Hemorrhagic syndrome |
20,5% |
25,0% |
|
Cholestatic syndrome |
31,1% |
65,0% |
|
Rashes |
0,0% |
15,0% |
|
Skin itching |
44,4% |
65,0% |
|
Severe jaundice |
44,4% |
75,0% |
|
Splenomegaly |
33,3% |
50,0% |
|
Ascites |
6,7% |
20,0% |
|
Anemia |
13,3% |
30,0% |
Clinical manifestations of HBV and unverified hepatitis are presented in Table 1. It shows that intoxication syndrome, including fever, weakness with unverified hepatitis was observed in 85%, while with HBV only in 46.7% of patients. In most cases, acute viral hepatitis B proceeds without fever, and in our case, an increase in temperature during HBV was observed in almost half of the examined patients, which could be associated with the presence of HSV. Asthenic syndrome with manifestations of sleep disturbance and pain syndrome (pain in the upper right quadrant) were expressed in both groups (more than 95%). Arthralgic syndrome was recorded in both groups with almost the same frequency (24.4% and 25%).
Catarrhal, dyspeptic and hemorrhagic syndromes were more common with unverified hepatitis than with HBV. Only three patients with unverified hepatitis had rashes in the form of vesicles, mainly on the lips, on the oral mucosa, which accounted for 15%, while according to the literature data, a rash appeared in almost 44% of cases [2,5].
All patients in the observed groups had hepatomegaly with varying degrees of enlargement (from 1.0 to 3.0 cm), splenomegaly in 50% with unverified hepatitis and in 15 patients (33.3%) with HBV. Cholestatic syndrome, including intense jaundice, skin itching, was 1.5-2 times more common in patients with unverified hepatitis (65-75%) compared to patients with HBV (31.1-44.4%). Ascites was observed more often with unverified hepatitis (20%) than with HBV (6.7%).
The analysis of biochemical data showed that in both groups of hepatitis there was a high level of activity of alanine aminotransferase (ALT) and aspartic aminotransferase (AST), a pronounced increase in total bilirubin due to direct was observed in patients with unverified hepatitis in comparison with patients with HBV (Fig. 2).
On fig. 2 shows the level of bilirubin in patients with HBV and unverified hepatitis. When comparing these two lines, it is clearly seen that the level of bilirubin in unverified hepatitis is higher and persists much longer than in HBV.
It is known that the severity of viral hepatitis is a change in the coagulogram, especially the prothrombin index (PTI) and prothrombin time (PT). In our patients, PTI decreased in 14 patients with HBV (31%), and in 8 patients with unverified hepatitis (40%), respectively.
Consequently, unverified hepatitis in the studied patients proceeded more severely and longer in time in comparison with HBV. Our patients underwent clinical, biochemical and serological studies. All patients with HBV had positive HbsAg, antibodies to Hbcor IgM. In patients with unverified hepatitis, viral hepatitis markers were negative. In order to exclude autoimmune hepatitis, appropriate tests were taken, the result of which was negative.
In addition to these tests, markers of herpes simplex viruses (HSV) were determined in all patients. Positive IgM was found in only 2.2% of the studied patients with HBV, but significantly high levels of IgG were detected in 90-91.1% of cases of all hepatitis.
From this it follows that the data of our study coincide with the literature data that more than 90% of the total population suffer from the herpes simplex virus. Among the studied patients, only 2% had an acute form of HSV, the remaining 90% of patients had a latent form of HSV. The presence of antibodies – IgM immunoglobulins, as well as an increase in the titer of IgG antibodies does not indicate a primary infection, since they can occur during reactivation. However, to identify carriers of HSV and persons in remission, it is necessary to carry out serological methods of research [8].
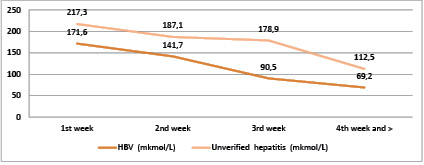
Fig. 2. Indicators of total bilirubin in patients with HBV and unverified hepatitis (weeks)
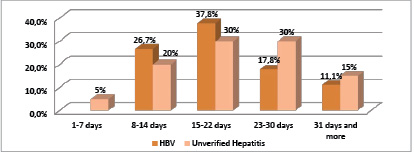
Fig. 3. Length of stay of patients in the hospital
As can be seen in Figure 3, the length of stay in the hospital for patients with HBV ranged from 8 to 50 days (≈20 days). And the length of stay of patients with unverified hepatitis in hospital treatment ranged from 7 to 56 days (≈23 days), which, apparently, was due to the severe course of the disease.
All patients of both groups received pathogenetic, detoxification, symptomatic therapy. In addition, patients with a severe form with high titers of antibodies to HSV were prescribed antiviral therapy (zovirax, acyclovir). In 20% of patients, while taking acyclovir, a positive trend was noted: a significant decrease in intoxication, jaundice, improvement in laboratory and biochemical parameters (decrease in bilirubin and transaminase activity, normalization of the coagulogram). Timely prescribed treatment with acyclovir can lead to a favorable outcome of herpetic hepatitis, which determines the importance of improving the clinical and laboratory diagnosis of this disease [7,9]. According to the literature, the survival rate among patients treated with acyclovir is higher than in those who did not receive it (88% versus 51%) [10].
Conclusions
Conducting a comparative clinical and laboratory characteristic of HBV and unverified hepatitis in persons infected with HSV, the following conclusions can be drown:
1. It has been reliably proven that 90% of observed patients are infected with HSV.
2. Acute viral hepatitis B and unverified hepatitis in persons infected with HSV occurs in most cases in a moderate form.
3. Fever with unverified hepatitis was observed in most cases (85%), which could be associated with the combined course of HSV.
4. It is possible that HSV infection can lead to severe adverse outcomes for both HBV and unverified hepatitis.
5. Mandatory examination for HSV (ELISA, PCR) is required for all patients with HBV and unverified hepatitis.
6. Timely administration of acyclovir against the background of generally accepted methods of treating acute viral hepatitis can lead to a favorable outcome of the disease.
Библиографическая ссылка
Иманбаева Л.А., Буранчиева А.А. CLINICAL AND EPIDEMIOLOGICAL CHARACTERISTICS OF THE COURSE OF ACUTE VIRAL HEPATITIS B AND UNVERIFIED HEPATITIS IN PERSONS INFECTED WITH THE HERPES SIMPLEX VIRUS // European Journal of Natural History. 2022. № 4. ;URL: https://world-science.ru/ru/article/view?id=34280 (дата обращения: 05.07.2026).
DOI: https://doi.org/10.17513/ejnh.34280