

The medical and social significance of miscarriage and its effect on the perinatal morbidity and mortality rates, as well as on the reproductive health of women places scientific and clinical research in this area among the most important objectives of modern medicine [1].
The analysis of miscarriage incidence in the Kyrgyz Republic has revealed a high level of reproductive loss, especially in terms of 6–12 and 28-36+6 weeks of gestation, which requires further work to identify risk factors and to develop predictive measures of great relevance and applied significance across the country [2].
Over the years the relationship between low dietary folate intake, hyperhomocysteinemia in pregnant women and the risk of obstetric and perinatal complications has been actively studied all over the world. In this regard, is the issue on the involvement of the folate metabolism genepolymorphisms, folate deficiency and hyperhomocysteinemia caused by it to the miscarriage, fetoplacental insufficiency, preeclampsia, premature birth, intrauterinegrowth restriction and congenital malformationformation isof particular interest [3].
The inevitable miscarriage causes are so varied that, until now, the creation of single classification is difficult. The issue on the beginning and scope of spousesurvey is widely debated in the literature. It is generally accepted abroad that a detailed examination should be started after three repeated miscarriages, in the Russian obstetrics it is recommended after two, but more and more scientists have noted the need to examine spouses even after one miscarriage.According to modern concepts, the miscarriage problem cannot be solved only during pregnancy. To ascertain any miscarriages causes and to assess the state of spouses’ reproductive system it is necessary to conduct comprehensive examination outside the state of pregnancy. The development of new high-tech diagnostic approaches aimed at the early, pre-symptomatic identification of high-risk married couples for miscarriageisof particular importance [4].
Considering the insufficient study of this issue in the Kyrgyz Republic, the study of significance of the genetic factor as a predictor of reproductive loss in women with miscarriage for modern obstetrics is of great scientific interest.
The goal of research is to study the predictive significance of nucleoid transitions in folate cycle genes during miscarriage.
Materials and research methods
Over the 2015to 2017period a cohort prospective study was conducted on the basis of the National Center for Maternal and Child Welfare (NCMCW) of the Ministry of Health of the Kyrgyz Republic.
The study involved 127 pregnant women, of them: the treatment group consisted of 74 women with miscarriage in history and the control group – 53 conditionally healthy women.
Table 1
Sample number (n)
|
Treatmentgroup, n = 74 |
Controlgroup,n = 53 |
||||
|
“-/-” |
“-/+” |
“+/+” |
“-/-” |
“-/+” |
“+/+” |
|
n = 9 |
n = 44 |
n = 21 |
n = 39 |
n = 12 |
n = 2 |
Table 2
Folate cycle gene characteristics
|
Abbreviation |
Locus |
Protein product |
Polymorphism |
|
MTHFR |
1р36.3 |
Methylenetetrahydrofolatereductase |
С677Т (А222V) |
|
А1298С (Е429А) |
|||
|
MTR |
1q43 |
Methioninesynthetase |
А2756G(D919G) |
|
MTRR |
5р15.3-15.2 |
Methioninesynthasereductase |
А66G(I22M) |
Table 3
Abbreviated notation of nucleoid pattern carriage in MTHFR, MTR and MTRR genes
|
Abbreviation |
Polymorphism |
Genotypes |
Abbreviatednotation |
|
MTHFR |
С677Т(А222V) |
С/С |
“-/-” |
|
С/Т |
“-/+” |
||
|
Т/Т |
“+/+” |
||
|
А198С (Е429А) |
А/А |
“-/-” |
|
|
А/С |
“-/+” |
||
|
С/С |
“+/+” |
||
|
MTR |
А2756G(D919G) |
А/А |
“-/-” |
|
А/ G |
“-/+” |
||
|
G /G |
“+/+” |
||
|
MTRR |
А66G(I22M) |
А/А |
“-/-” |
|
А/ G |
“-/+” |
||
|
G /G |
“+/+” |
Depending on the nucleoid pattern carriage in folate cycle genes, pregnant women were divided into subgroups (Table 1).
The average age of women of the treatment group was 29.9 ± 2.5 per 100 examined, control groups – 29.1 ± 2.5, respectively, the groups were comparable, no statistically significant difference was found in groups, p > 0.005.
To identify the significance of gene polymorphism in women with reproductive losses, the folate cycle gene examination was conducted (Table 2): three folic acid metabolism genes, MTHFR, MTR and MTRR, associated with hyperhomocysteinemia and folivododeficiency states were examined.
The nucleoid pattern inMTHFR, MTR and MTRR genes were determined by the PCR method (allele-specific polymerase chain reaction) with result detection in real time.
Table 3 provides the information on abbreviated notationsof detected nucleoid patterncarriage.
The required sample number was calculated according toE.N. Shigan (1987) (t = 3.2, P < 0.001, 99.9 %) [5].
Calculations of relative values (P) and their errors (mp) have been made. To estimate the relative ratio numerical value difference confidence the calculation of confidence criterion (confidence coefficient, Student’s t-test and χ2) recommended by N.E. Chernova has been made (2006) when conducting medical and social research using the formula  , under t = 3.2 the differenceprobability is 99.9 % or the difference confidence is < 0.001 [5].The error significance criteria were selected as error-free prediction probability values – less than 5 % bilateral (p < 0.05), with 95 % confidence interval and statistical power – 80 % power. The rank significance was estimated by the Spearman rank correlation ratio under the formula:
, under t = 3.2 the differenceprobability is 99.9 % or the difference confidence is < 0.001 [5].The error significance criteria were selected as error-free prediction probability values – less than 5 % bilateral (p < 0.05), with 95 % confidence interval and statistical power – 80 % power. The rank significance was estimated by the Spearman rank correlation ratio under the formula:
To carry out statistical processing of obtained data, the online free software package of the U.S. Center for Disease Control OpenEpi 3.03 has been used.
The authors declare no conflict of interest in the Article.
Research results and discussion
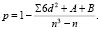
It was in research revealing that the polymorphism of nucleoids in MTHFR gene in position 677 of folate cycle prevailed in the group of women with miscarriage (main group, n = 74); table 1 presents data as a triangle with a narrow base shifted toward heterozygous transition (C / T), for healthy women (control group, n = 53) – the data are presented in a form of triangle with narrow base, which emphasizes the absence of mutations in a larger number of examined patients, p < 0.001. However, the nucleoidtransition by heterozygous type has been revealed in 22.6 ± 5.8 per 100 examined women in the control group.
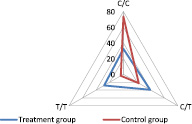
Fig. 1. MTHFRgene polymorphism in the position 677 of folate cycle
Fig. 2 presents the data of MTHFR folate cycle polymorphism in the position 1298, and the larger number of women with the nucleoid pattern inherent in this position (A / A – 75.5 ± 5.9 per 100 women) were revealedin the control group; triangle is represented by a narrow base with a broad base; for the treatment group the data look like as the triangle with a broad base, elongated towards homozygous mutation (C / C – 41.9 ± 5.7 per 100 women), p < 0.001.
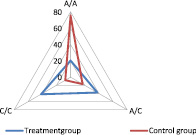
Fig. 2. MTHFR gene polymorphism in the position 1298 of folate cycle
For the MTR folate cycle in the position 2756 in the control group, the nucleoid pattern A / A revealed in 79.3 ± 5.6 per 100 women is also statistically significantly more frequent, and the data are presented as a triangle elongated upwards (Fig. 3), this pattern in the treatment group was detected only in 27.0 ± 5.2 per 100 women, p < 0.001. According to the treatment group data, the triangle is represented as a broad base with prevailed G / G mutation (37.8 ± 5.6 per 100 women examined), which is statistically significantly more frequent in the control group (7.6 ± 3.6 respectively), p = 0.003.
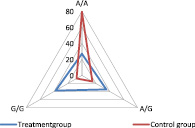
Fig. 3. MTHFR gene polymorphism in the position 2756of folate cycle
The similar pattern has been also detected for MTRR gene in the position 66 of folate cycle (Fig. 4), and the triangle with a narrow base and an elongated vertex is inherent in the control group, where nucleoids in 83.0 ± 5.2 women per 100 women are represented by the A / A pattern, which is statistically significantly more often than the treatment group (12.2 ± 3.8, respectively), p < 0.001. For the treatment group, the data demonstrate the triangle with elongated base towards homozygous G / G transition, which is statistically significantly more often in the group of women with miscarriage (treatment group – 51.4 ± 5.8 per 100 examined women) than in the control group (5.7 ± 3.2 respectively), p < 0.001.
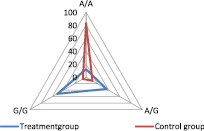
Fig. 4. MTHFR gene polymorphism in the position 66of folate cycle
The data of folate cycle gene nucleoid pattern in the women of comparison groups are presented more clearlyin Fig. 5. The graphic in the women of control group looks like a star, the rays of which are represented in more than 80 % of women with the inherent nucleoid patternfor this gene. Mutated genes have been detected in every 5th woman and are presented in various combinations. For the treatment group, the graphic looks like a square with elongated angle in the MTRR gene of G / G transition mutation.
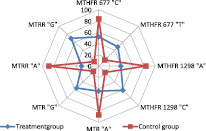
Fig. 5. Combinationoffolate cycle polymorphic genemodels in women DNA
The obtained data enable us to distinguish thefolate cycle gene nucleoid transitions in significant risk factors for miscarriage, especially if these mutations were homozygous. Considering the large importance of folate cycle in cell division of developing embryo, it is necessary to detect timely this risk factor and to level its action by taking folic acid, and, if necessary, by folates at the planning pregnancy stage of women at risk.
Further, the study has examined the significance of various modifications of folate cycle gene models depending on the presence or absence of homozygous and heterozygous transitions into them (Table 4). The average age of women with miscarriage was 29.9 ± 2.5 per 100 women examined.
Comparing reproductive losses depending on the genotype model, we have identified three different groups: “- / -” – homozygous normal genotype (9 women), “- / +” – heterozygous gene transition (44 women) and “+ / +” – homozygous gene transition (21 women). The most numerous group had various heterozygous combinations of nucleoid transition in the folate cycle genes – 59.5 ± 5.7 per 100 women, which is statistically significantly more compared to the group “- / -” with homozygous genotype without nucleoid transitions (12.2 ± 3.8 per 100 women), t = 6.9, p < 0.001, and than in the group with homozygous nucleoid transition (28.3 ± 5.2, respectively), t = 4.0, p < 0.001. In addition, it should be noted that every fifth woman with miscarriage has shown the homozygous transition “+ / +”, which is statistically significantly more frequent than “- / -” – homozygous normal genotype, t = 2.5, p = 0.01.
Describing the women with homozygous normal pattern of folate cycle genes, it should be noted that in 100 % of cases there was a single reproductive loss in history, the statistically significant difference with the group of heterozygous transitions p = 0.01.
The single fetal loss was recorded in 29.6 % of women in the group of women with heterozygous nucleoid transition, and double reproductive losseswere recorded in70.5 %, and the statistically significant difference in losses was revealed, p < 0.001. Thus, the transitions of nucleoids of heterozygous type are predictors of miscarriage; obtained data indicate the need to include women with this transition in the risk group of miscarriage.
It follows on the obtained data that the worst is the group with homozygous transition of nucleoids. In 100 % of cases in such women there is fetal loss in three or more pregnancies in succession, while this pathology has not been detected in the first two groups.
Considering the stages of pregnancy at reproductive losses in the group of women with the homozygous model “- / -” of standard nucleoid pattern, the rank places are presented in decreasing form as follows: up to 12 weeks (44.4 %), 13-21 weeks (22.2 %) 22-31 weeks (22.2 %) and 32 weeks or more (11.2 %).
The rank places in the group with heterozygous nucleoid pattern “- / +” are presented in a different way, in decreasing order: 13-21 weeks (72.7 %), up to 12 weeks (20.4 %), 22-31 weeks (4.6 % ) and 32 weeks or more (2.3 %).
For the group with homozygous nucleoid transition “+ / +”, the rank places are presented as follows: 13-21 weeks (66.7 %), up to 12 weeks (19.1 %) and 22-31 weeks (14.3 %), this group of the pregnancy stages in this group were interrupted up to 32 weeks.
The pregnancy was interrupted statistically significantly less often in the stages of 13-21 weeks in the group with the normal nucleoid pattern “- / -” in comparison with the group of heterozygous aberrations “- / +” (p < 0.01) and homozygous transitions “+ / +” < 0.05).
The obtained data enable us to distinguish the critical stages of pregnancy termination – 13-21 weeks typical for folate cycle polymorphic genes.
Further, during the study we have examined the gestation course features in women with miscarriage in history (Table 5); as mentioned above, the average age of women in the treatment group was 29.9 ± 2.5 years and of the control group 29.1 ± 2. 5 years, no statistically significant difference was found in groups, p > 0.05; groups are comparable.
Hyperhomocysteinemia was detected in 36 women (48.6 %) of the group and 2 (3.8 %) women of the control group, p < 0.001. Hyperhomocysteinemiain the treatment group was statistically significantly more frequent in thegroup “+ / +” – in 85.7 % of women as compared to thegroup “- / +”– 36.4 % of cases, t = 4.7, р < 0,001 andgroup “-/-” – 22,2 %, t = 4,0, р < 0,001. Hyperhomocysteinemia in the treatment group was also statistically significantly more frequent in thegroup “+ / +” – 50.0 % of cases as compared to the group “- / +” – 8.3 %, p < 0.001, and in the group “- / -” this pathology was not registered.
The aggravated obstetric history has been revealed in 43 (58.1 %) women, while reproductive losses were not included in theburdened obstetric history; this ratio has not been registered in the control group. In the treatment group in 100.0 % of cases, it was aggravated in the women of thegroup “+ / +”, which is statistically significantly more frequent than thewomen of the group “- / -” (33.3 %), t = 4.3, p < 0.001 and the group “- / + “(43.2 %), t = 7.6, p < 0.001.
Table 4
Reproductive losses in women with miscarriage, depending on the presence
of mutations in the folate cycle gene models
|
Treatment group |
||||||
|
“–/–”, n = 9 |
“–/+”, n = 44 |
“+/+”, n = 21 |
||||
|
Abs. |
Р ± mр |
Abs. |
Р ± mр |
Abs. |
Р ± mр |
|
|
Averageage, years |
29,9 ± 2,5 |
|||||
|
Reproductivelosses, number: |
||||||
|
- one (1) |
9 |
100,0 ± 0,0 |
13 |
29,6 ± 6,9*** |
- |
- |
|
- two (2) |
- |
- |
31 |
70,5 ± 6,9 |
- |
- |
|
- threeormore(3 and>) |
- |
- |
- |
- |
21 |
100,0 ± 0,0 |
|
Gestational age at miscarriage, weeks: |
||||||
|
- up to 12 weeks |
4 |
44,4 ± 16,6 |
9 |
20,4 ± 6,1 |
4 |
19,1 ± 8,6 |
|
- 13-21weeks |
2 |
22,2 ± 13,9 |
32 |
72,7 ± 6,7** |
14 |
66,7 ± 10,3* |
|
- 22-31weeks |
2 |
22,2 ± 13,9 |
2 |
4,6 ± 3,1 |
3 |
14,2 ± 7,6 |
|
- 32 and more weeks |
1 |
11,2 ± 10,5 |
1 |
2,3 ± 2,3 |
- |
- |
Note: statistical significance of differences *р < 0,05, **р < 0,01,***р < 0,001 between groups.
Table 5
Gestation course features depending on nucleoid pattern in folate cycle genes
|
Treatment group |
Контрольная группа |
|||||||||||
|
“-/-”, n = 9 |
“-/+”, n = 44 |
“+/+”, n = 21 |
“-/-”, n = 39 |
“-/+”, n = 12 |
“+/+”, n = 2 |
|||||||
|
Abs. |
Р ± mр |
Abs. |
Р ± mр |
Abs. |
Р ± mр |
Abs. |
Р ± mр |
Абс. |
Р ± mр |
Абс. |
Р ± mр |
|
|
Averageage, years |
29,9 ± 2,5 |
29,1 ± 2,5 |
||||||||||
|
Hyperhomocysteinemia |
2 |
22,2 ± 13,9*** |
16 |
36,4 ± 7,3*** |
18 |
85,7 ± 7,6 |
- |
- |
1 |
8,3 ± 8,0*** |
1 |
50,0 ± 35,4 |
|
Burdenedobstetrichistory |
3 |
33,3 ± 15,7*** |
19 |
43,2 ± 7,5*** |
21 |
100,0 ± 0,0 |
- |
- |
- |
- |
- |
- |
|
Somatic pathology: |
2 |
22,2 ± 13,9*** |
14 |
31,8 ± 7,0*** |
28 |
133,3 ± 0,0 |
11 |
28,2 ± 7,2*** |
9 |
75,0 ± 12,5 |
2 |
100,0 ± 0,0 |
|
- anemia |
2 |
22,2 ± 13,9*** |
12 |
27,3 ± 6,7*** |
21 |
100,0 ± 0,0 |
11 |
28,2 ± 7,2*** |
9 |
75,0 ± 12,5 |
2 |
100,0 ± 0,0 |
|
- arterialhypertension |
- |
- |
1 |
2,3 ± 2,3*** |
4 |
19,1 ± 8,6 |
- |
- |
- |
- |
- |
- |
|
- varicoseveinsepidermally |
- |
- |
1 |
2,3 ± 2,3*** |
3 |
14,2 ± 7,6 |
- |
- |
- |
- |
- |
- |
|
Pregnancycomplications (anamnesis): |
- |
- |
36 |
81,8 ± 5,8*** |
42 |
200,0 ± 0,0 |
- |
- |
3 |
25,0 ± 12,5*** |
3 |
150,0 ± 0,0 |
|
- PTSDPost-Traumatic Stress Disorder |
- |
- |
11 |
25,0 ± 6,5** |
16 |
76,2 ± 9,3 |
- |
- |
2 |
16,7 ± 10,8*** |
1 |
50,0 ± 0,0 |
|
- threatened spontaneous miscarriage |
- |
- |
21 |
47,3 ± 7,5*** |
17 |
81,0 ± 8,6 |
- |
- |
1 |
8,3 ± 8,0*** |
2 |
100,0 ± 0,0 |
|
Fetalcongenitalanomalies |
- |
- |
4 |
9,1 ± 4,3** |
9 |
42,9 ± 10,8 |
- |
- |
- |
- |
- |
|
Note: statistical significance of differences *р < 0,05, **р < 0,01,***р < 0,001 in comparison with the group “+/+”.
The somatic pathology was detected in 44 women (59.5 %) of the treatment group and in 22 women (41.5 %) of the control group, and the statistically significant difference was: t = 2.0, p = 0.04. At the same time, in the treatment group at “- / -” the pathology was detected in 2 women (22.2 %), which is statistically significantly less frequently than the group “+ / +”, where somatic diseases were registered in 28 women (133.3 %), namely, 1.3 somatic pathologies have fallen on one woman, t = 8.0, p < 0.001. In thewomen group “- / +”, this pathology was detected in 14 women (31.8 %), which is statistically significantly less often than in the group “+ / +”, t = 14.5, p < 0.001.
The somatic pathology in the control group was also detected statistically significantly more often in the group “+ / +” in 2 women (100.0 %) compared with thegroup “- / -” in 11 women (28.2 %), t = 10.0, p < 0.001 and in thegroup “- / +” in 9 women (75.0 %).
The following diseases were revealed in the structure of women’s somatic pathology: anemia, arterial hypertension and varicose veins of lower limbs.
Only anemia with a different nucleoid pattern of folate cycle genes was detected in the treatment group women in the somatic pathology structurein 100 % of cases.
In the treatment group with normal homozygous pattern “- / -” the somatic pathology is also represented only by anemia (22.2 ± 13.9 per 100 women); no statistically significant difference with the control group (28.2 ± 7.2 respectively) is established, t = 0.4, p = 0.7.
Under the gene type “- / +” in the treatment group, the somatic pathology structure is presented as a decrease: anemia (27.3 %), arterial hypertension (2.3 %) and varicose veins of lower limbs (2.3 %), and the statistically significant prevalence of anemia compared with another pathology has been revealed, t = 3.5, p < 0.001. In comparison with the control group “- / +” (75.0 %), the statistically significant difference has been also revealed, t = 3.4, p = 0.001.
The somatic pathology was detected statistically significantly more often in the treatment group “+ / +” in 28 cases, i.e. one woman had 1.3 diseases each and the structure is presented as a decrease: anemia (75.0 %), arterial hypertension (14.2 %) and varicose veins of lower limbs (10.7 %). The statistically significant difference has been established between detected anemia (100.0 ± 0.0 per 100 women) and arterial hypertension (19.1 ± 8.6, respectively), t = 9.4, p < 0.001 and varicose veins of lower limbs (14, 2 ± 7.6, respectively), t = 11.3, p < 0.001. In the treatment and control groups by homozygousnucleoid pattern “+ / +” anemia has been detected in 100.0 % of cases, p > 0.05.
Considering the gestation complicationsin examined women, it should be noted that 78 complications were revealed in the treatment group, whereas only 6 complicationswererevealed in thecontrol group, p < 0.001.
Herewith, no complications were revealed in women with the homozygous normal nucleoid pattern “- / -” in both groups.
36 complications were revealedin the treatment group with theheterozygous pattern “- / +”, which is statistically significantly more than in the control group (3 complications), p < 0.001.
The worst situation turned out to be under the homozygousnucleoid pattern “+ / +” in folate cycle genes; during the study, 42 complications were revealed in the treatment group, i.e. 2.0 complications per woman, which is statistically significantly more often than in the control group (3 complications), p < 0.001.
According to the complication structure, they were revealed in the treatment group were identified by decreasing: threatened spontaneous miscarriage, severe preeclampsia and congenital malformations of fetus / newborn. Comparing the treatment group women by heterozygous and homozygous polymorphism of nucleoids, it should be noted that the risk of spontaneous miscarriage was statistically significantly more frequent in the latter (“- / +” – 47.3 % and “+ / +” – 81.0 %), t = 4.5, p < 0.001, severe preeclampsia (“- / +” – 25.0 % and “+ / +” – 76.2 %), t = 3.0, p = 0.004 and congenital anomalies of fetus / newborn (“- / +” – 9.1 % and “+ / +” – 42.9 %), t = 2.9, p = 0.005.
The control situation in the group has turned out similar; pregnancy complications have been revealed significantly more frequent in women with homozygous polymorphism, p < 0.001, but no congenital abnormalities of fetus were revealedin this group. In the group “- / +”, two cases of severe preeclampsia were detected (16.7 %), and in the group “+ / +” – one case (50.0 %); statistically significant difference was t = 3.1, p = 0.01. In addition, one case of spontaneous miscarriage was revealed in the group with heterozygous pattern of folate cycle polymorphism”- / +” (16.7 %), and in the group with homozygous pattern “+ / +” – in two women (100.0 %) The statistically significant difference was t = 11.5, p < 0.001.
Thus, during the study it was established the following:
1. The nucleoid pattern in folate cycle genes in women with miscarriage differs from the control group, and the difference is statistically significant, p < 0.001.
2. Homozygous transition of nucleoids is more often detected in the treatment group in comparison with the control group, p < 0.001.
3. Heterogeneous gene transitions are more frequentlyin women with miscarriage(59.5 %), p < 0.001.
4. The triple reproductive loss is typical forhomozygous transition of nucleoids, which is the worst version of gene carriage and is important in predicting miscarriage.
5. Heterozygous transition of nucleoids also plays a significant role in miscarriage, since such gene pattern is established in women with one-time and two-time fetus loss, p < 0.001.
6. The single reproductive loss has been detected with the normal homozygous-type nucleoid pattern, p < 0.001.
7. The critical stages of pregnancy termination for homozygous transitions were the period up to 12 weeks (44.4 %), for heterozygous – 13-21 weeks (72.7 %) and for the normal gene pattern – 13-21 weeks (66.7 %) p < 0.001.
8. Hyperhomocysteinemia was revealed statistically significantly more often in the homozygous transition group in comparison with another gene pattern, both in the treatment group and in the control group, p < 0.001.
9. The aggravated obstetric history has been revealed in 58.1 % of women with miscarriage, statistically significantly more often in the group with homozygous transition, p < 0.001.
10. No gestation complications were revealed in women of both groups with the normal homozygous nucleoid pattern, p > 0.05.
11. The worst situation has been revealed statistically significant in women with homozygous nucleoid transition as compared to other groups, p < 0.001.
Conclusion
The analysis of various nucleoid transitions in folate cycle genes has enabled to reveale the important role of genetic predisposition in predicting miscarriage, and the worst outcome was in women with homozygous nucleoid transitions. Considering the data obtained in the study, at the stage of pregnancyplanning it is necessary to reveal timely the miscarriage predictors and to level their action by taking folates for prolongation and reduction of gestation complications.